The science behind LASIK
- The human eye is a remarkable organ, enabling light from the environment to enter, focusing it on a “screen” at the back of the eye, and enabling the sense of sight, with our brains producing full color images.
- However, flaws in our eye impede our ability to focus the light from point-like objects to “points” on our retinal screens, requiring corrective lenses to bring those blurry images into focus.
- LASIK is a breakthrough medical intervention that, for some people, helps them live lives free of glasses or contact lenses, yet still see perfectly. Here’s what anyone considering it should know about the science behind it.
The human eye is one of the most remarkable organs that each of us is equipped with. As we open our eyes, our pupils allow light from the environment to enter, providing us with a visual window into the outside world. That light gets focused by a lens within our eye, where muscles and ligaments can control the position and shape of that lens. Then, that focused light arrives on a screen-like organ located at the back of our eyeballs: the retina, which uses photodetectors — rods and cones — to process that light signal and send it to our brains. Our brains then interpret the full suite of data to produce an image. When the whole system works together, it produces the experience of sight: one of what’s commonly known as “the five senses,” although in reality, humans have many other senses as well.
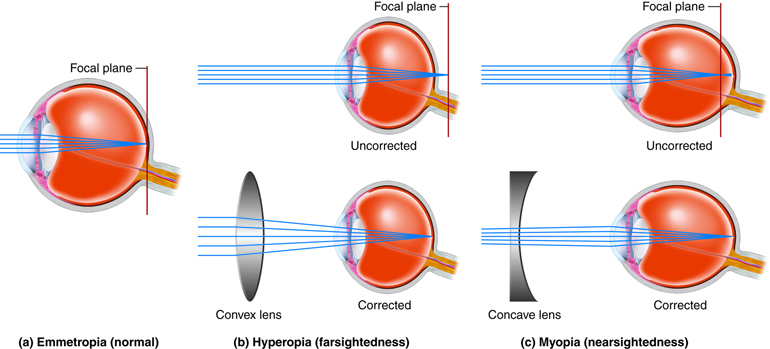
Unfortunately, our eyes aren’t infallible, perfect organs that always focus the light down to a point on our retinas. Some of us struggle to focus objects that are located too close to us, rendering us farsighted. Others struggle to see objects located too far away, rendering us nearsighted. Some of us have both of these afflictions, particularly beyond the age of 40-to-50. And some of us have an astigmatism: where the light from external objects isn’t focused down to a point, but rather to a distorted, elliptical-like shape.
For hundreds of years, corrective lenses in the form of eyeglasses were our only option. In the 20th century, contact lenses became widespread, as plastics and hydrogels revolutionized comfort and wearability. But now, a new option has emerged: LASIK, a form of laser eye surgery that has helped many millions of patients thus far. Here’s the science behind LASIK to help inform you as to whether or not you, or someone you love, might benefit from this transformative procedure.
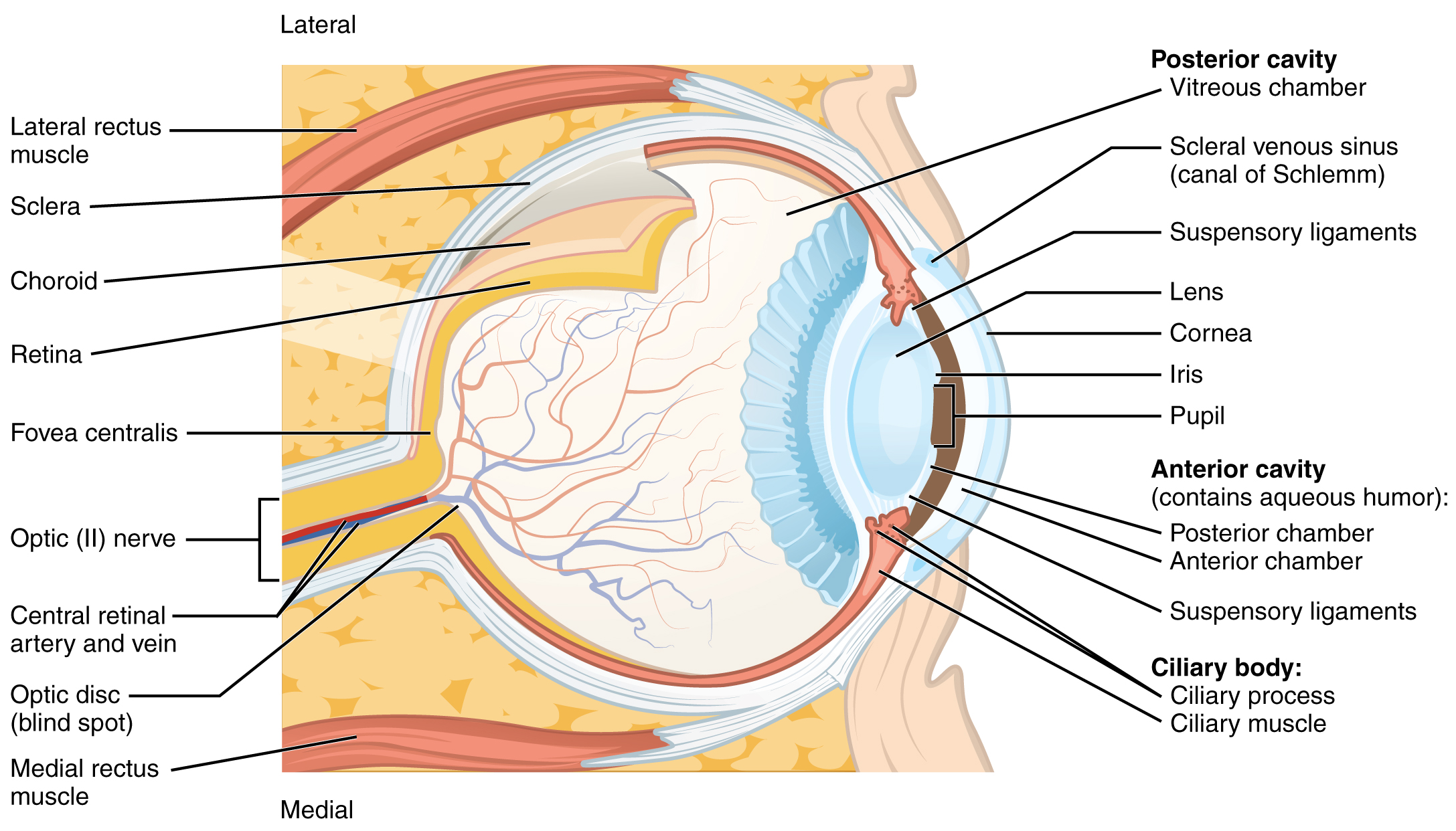
The first thing we should all understand is the basics of how your eyes actually work, and how the anatomy of your eye relates to your sense of vision: i.e., what you actually perceive with your sight. Once your eyelids open, the first thing that the incoming light from the environment hits is your cornea: the outer, clear surface of your eyeball. Corneas are thin, clear layers that bend and focus external light toward your pupil, allowing light to enter your eyes. The light passes through your eye’s anterior cavity (full of fluid known as aqueous humor), and then enters your pupil. After that, it encounters the lens of your eye: the component of your eye that acts just like a glass lens, focusing that light toward a point.
The incoming, focused light is now going to enter the internal/rear chamber of your eyeball — known as the posterior cavity and filled with fluid known as vitreous humor — and then will encounter the retina: a screen on the internal back of your eyeball, filled with rods and cones, enabling us to detect light’s intensity and color. Finally, the rods and cones within your retina connect to your eye’s optic nerve, which sends those optical signals picked up by the rods and cones to your brain, which enable you to construct an image and experience the sensation of “seeing” with your eyes.
In an ideal human, under ideal circumstances, the anatomy of your eye allows to to perceive:
- light from a source,
- located a particular distance away from your eyeball,
- where that light comes in and enters your eye through your pupil,
- gets focused by your eye’s lens,
- so that the light comes to a focus at a point,
- where that point lands directly on your retinal tissue,
- and stimulates the appropriate rods and cones,
- enabling your brain to construct a clear, crisp, focused image.
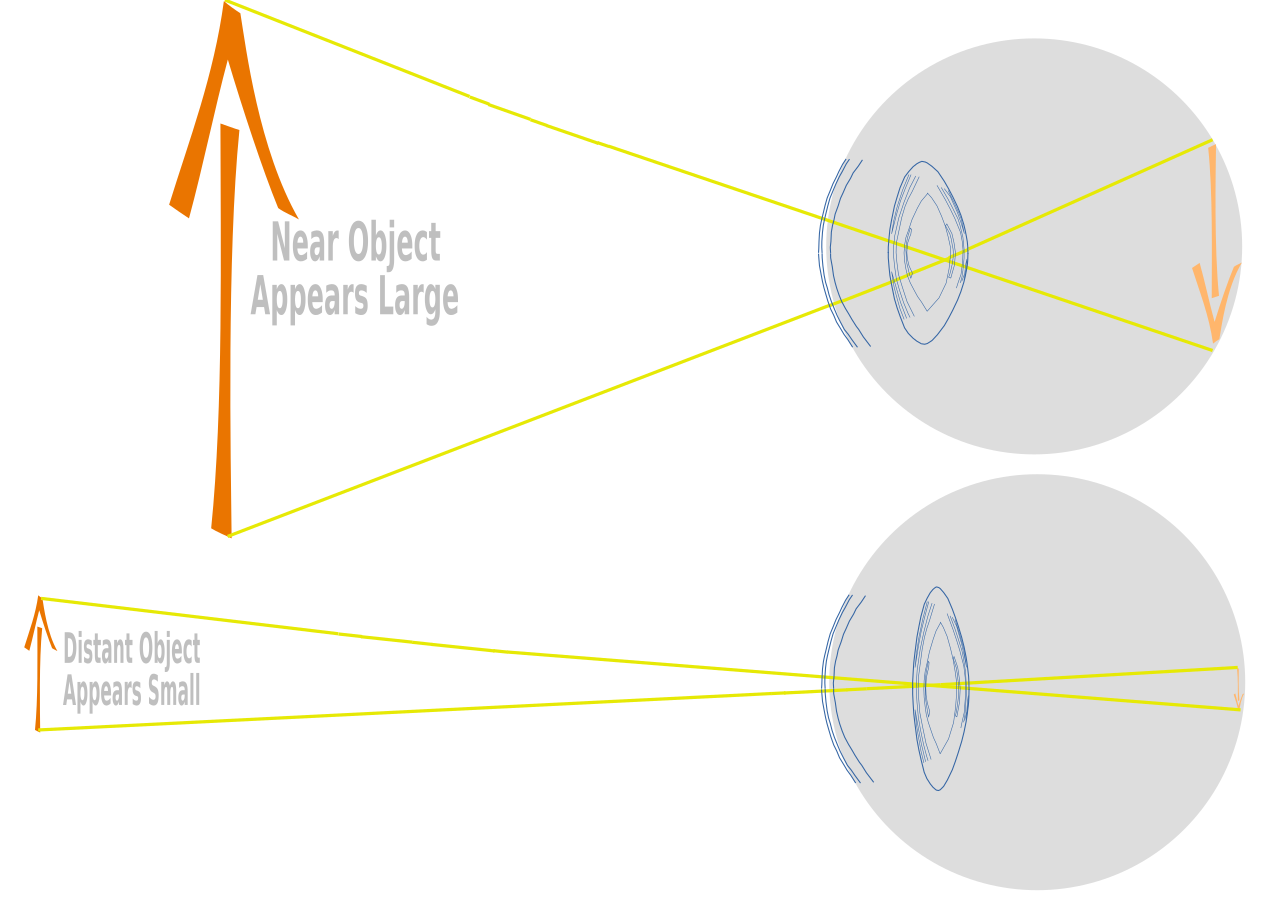
However, there are limitations to this process. If the light source is very close to your eyeball, your lens has to work very hard to converge that light quickly enough, over a short enough distance, that it comes to a focused point before it reaches your retina. If it converges after it hits your retina, it’ll produce a blurry image: a spread-out image, meaning that you can’t focus the light for objects that are too close.
Similarly, if the light source is very far away — even arbitrarily far away so that it can be approximated as infinitely far away, such as the Moon, planets, or stars — it’s very easy for your eye’s lens to focus the light too rapidly. Remember: your eye only has one lens, and it uses the same lens for focusing “near light” as “far light.” If the light focuses down to a point before it reaches your retina, then by the time it strikes your retina, you’ll see a blurry image once again: a spread-out image, rather than being focused to a clear image of the original.
Now, it isn’t just that you have one, unchanging eyeball with unchanging parts and components no matter whether you’re looking at something near or far. You can see this for yourself simply by holding up one finger in front of your face. When you hold up a finger in front of your face, you can:
- focus on the finger, which will become clear as you focus on it, while the objects in the background appear blurred,
- or you can focus on the faraway background objects, which will become clear as you focus on them, while your finger in the foreground appears blurred instead.
How does your eye do this? How does your eye “choose” which object to bring into focus?
If all you had was the same lens in the same configuration — with the same distance between your lens and your retina — for all objects that you’d look at, you’d disappointingly find that there was only one narrow “range” of distances that you could actually bring into focus with your eyes. Objects that were more distant would be de-focused, as that light would come to a focal point before it reached your eyes, while objects that were closer would also be de-focused, as that light wouldn’t come to a focal point until they had already passed your retina. The optical configuration of your eye, in order to focus on different objects with the same anatomy, must change depending on where you’re looking.
And this is something that your eyes can actually do! Your eye doesn’t take on a fixed shape, and neither does your eye’s lens. There are muscles and ligaments all around your eyes, including:
- the ciliary muscles near your eye’s lens,
- the suspensory ligaments that hold your lens in place,
- and the lateral and medial rectus muscles, which can extend or foreshorten the length of your eyeball.
(There are also inferior and superior rectus muscles, as well as inferior and superior oblique muscles.) When you view an object, these muscles work to try to co-optimize both the shape of your lens and the shape of your eyeball, so that the light that enters your eye — for the object you’re focusing on — gets focused down perfectly to a focal point that falls directly onto the rods and cones located on your retina itself.
However, there’s always a limit. You can bring your finger closer and closer to your eye(s), and at some point, it will start to blur; your “near point” isn’t infinitely near. The farther you have to place an object in order for your eyes to focus it, the more severely farsighted you are. For some of us, our “far point,” for an object located arbitrarily (or even infinitely) far away, can be focused to a point that will fall on our retinas. For others, however, there’s a maximum distance that we can crisply see an object at: a far point that isn’t infinitely far away. That’s what makes someone nearsighted, and the closer that “far point” is, the more severely nearsighted we are.

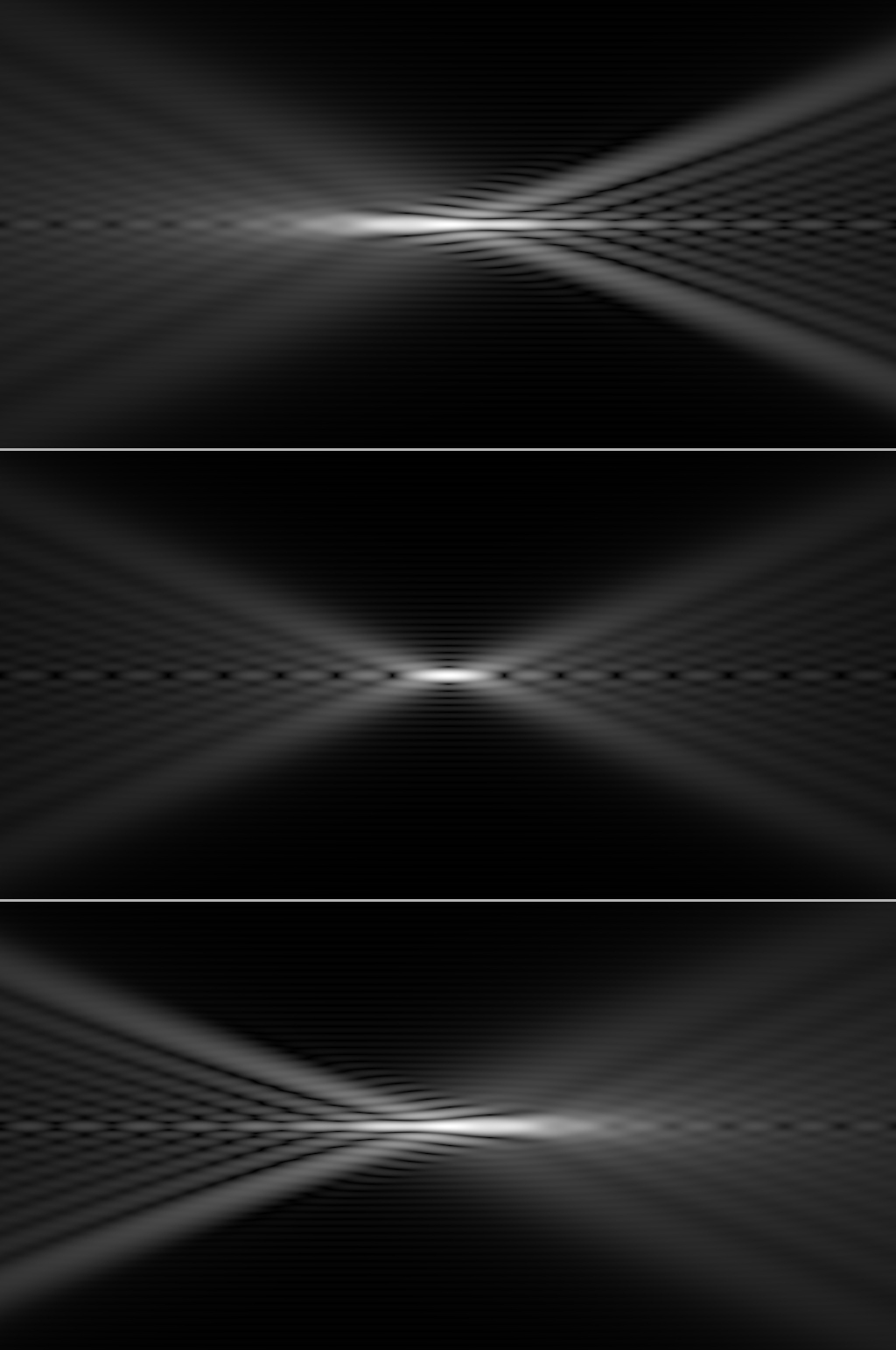
Finally, there’s the phenomenon of astigmatism: where instead of the incoming light from a circle producing a circle on your retina, it gets distorted differently in different directions. For example, if you imagine a “crosshairs” where you have a circle with a vertical and horizontal line running through the center, an astigmatism will create an image that is no longer perfectly symmetrical the way the circle-and-lines is symmetrical. There are three main classes of astigmatism, as follows:
- Myopic astigmatism: where in either the horizontal or vertical directions (or both), the incoming light gets focused in front of the retina, rather than on the retina, producing an image that’s always blurred in one or more dimensions.
- Hyperopic astigmatism: where in either the horizontal or vertical directions (or both), the incoming light gets focused behind the retina, rather than on the retina, producing an image that’s always blurred in one or more dimensions.
- Mixed astigmatism: where one axis (horizontal or vertical) is myopic (nearsighted) and one is hyperopic (farsighted) in the same eye, producing an image that’s blurred in two fundamentally different ways.
In addition to these three types, you can have an irregular astigmatism as well, where what optometrists call the “principal meridians” (an analogy of the crosshairs) aren’t horizontal and vertical, but rather are tilted at an angle: up to a maximum of 45°.
You can correct nearsightedness, farsightedness, astigmatism, or all three with corrective lenses. Typically, we use external lenses: lenses that are outside of our eyeballs themselves. Eyeglasses (that sit away from the eyes) are one option, and contact lenses (which come into contact with your external corneas) are the second option.
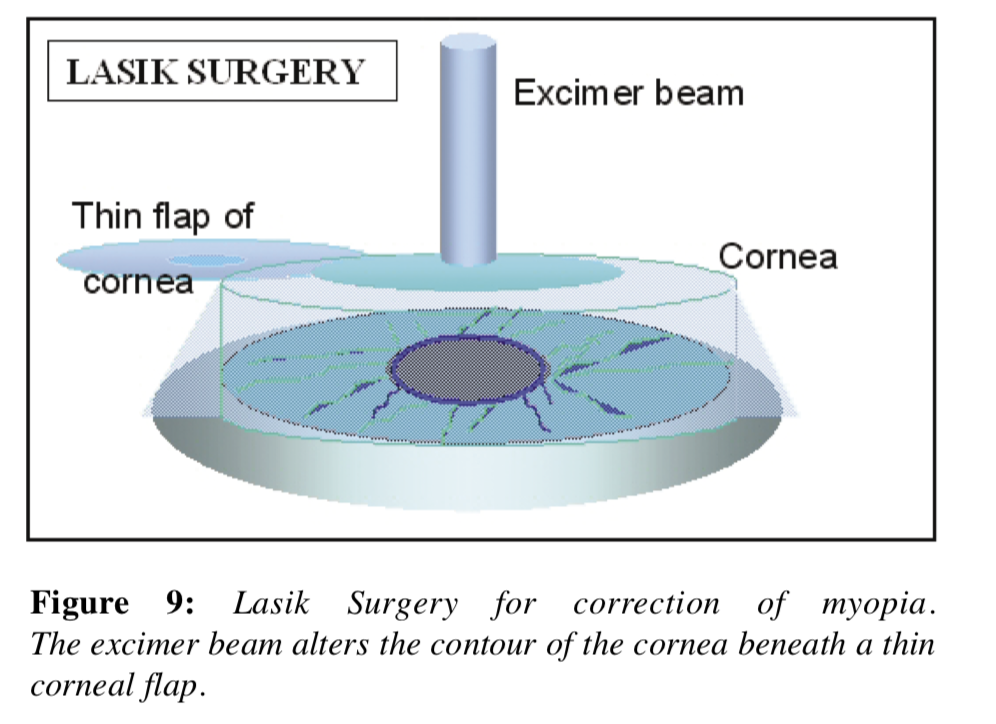
However, there are two surgical options that are available to many: LASIK (short for Laser-Assisted In Situ Keratomileusis), and PRK (short for Photorefractive Keratectomy). Both methods are forms of laser eye surgery, and both have comparable success rates and effectiveness for correcting vision. They both “add in” an additional, corrective lens before the light ever reaches your eye’s lens, by shaping a new one in your eye’s corneas.
The major difference in procedure is that, with LASIK, they cut a flap into your cornea and “carve” a new, corrective lens into your cornea’s interior, then fold the flap back over and let it heal. With PRK, there is no cutting, and instead they remove the top layer of your cornea and etch a new lens onto the underlying layer, then allowing the outer layer of your cornea to grow back and heal. These procedures differ in terms of pain/discomfort (PRK can be quite painful, LASIK is painless) and in terms of recovery time (LASIK is very fast, PRK is much slower).
It might seem like LASIK would be the option that everyone would choose, but whether you’re a good candidate for LASIK or not depends on your anatomy in a way that PRK doesn’t. Human corneas are relatively thin parts of your eye: typically only about half-a-millimeter thick, and subdivided into several layers. There’s a risk, if you attempt to cut a flap into someone’s cornea and their cornea is too thin, that instead of successfully making a flap that then gets folded back to enable the engraving of a lens, the top layer of the cornea can be accidentally removed entirely.
This is why the thickness of your cornea is one key to determining whether you’re a good LASIK candidate: if your cornea is ~500 microns thick or more, you’re likely an excellent candidate as far as corneal thickness goes. If your cornea is slightly thinner, you may still be a good candidate, but if your cornea is severely thinner (say, ~480 microns or less), most doctors will instead recommend PRK, or a variant of PRK known as ASA: Advanced Surface Ablation, which is sometimes called “flapless LASIK” for marketing purposes.
The largest downside of PRK (or ASA) is that they have long recovery times and often come along with much discomfort; the largest downside to LASIK is that sometimes there are recovery complications (dry eyes, “starring” of bright point sources of light, nighttime vision loss, etc.) that arise.
However, there are also two general types of risks associated with all types of laser surgery: LASIK, PRK, or ASA.
- Your eye needs to recover and readjust after any of these types of surgeries, and your lenses and muscles inside your eyes are going to work together to find a “new normal” in the aftermath of your surgery. In some cases (in a few percent of patients), this will mean that your eyes have adjusted to a new configuration where either your near point or your far point is sub-optimal, or where you still have a slight astigmatism. Follow-up “touch up” surgery, or going back to wearing corrective lenses, is often required.
- These surgeries can only add one additional lens — a lens fixed in its orientation and configuration — onto each eye. If you’re an adult whose vision has long been stable and continues to remain stable, this additional lens can provide you with tremendous benefits to your vision. However, if your vision has been steadily changing over time, it will likely continue to do so; corrective laser surgery doesn’t affect the rest of your eye’s anatomy, or the surrounding muscles which determine your eye’s shape. For those of us with regularly changing vision, laser eye surgery will likely offer only a very temporary reprieve from needing glasses or contacts.
The only other non-catastrophic (i.e., a laser malfunction occurred during surgery, or you somehow got the wrong person’s prescription lens etched into your eye) caveat that everyone should know about is this: if you’re getting laser surgery to correct nearsightedness, it likely means you will need reading glasses sooner than you would otherwise. LASIK, PRK, and ASA all offer no protective effects against the standard aging process, including the effect that your “near point” naturally will move back, farther away from your eyes, as you age; by your 40s, for most patients, you will most likely require reading glasses even after LASIK.
With all that said, however, the one thing you should make sure to do — after doing all of your homework about your vision and your options — is to speak with a qualified medical professional: either an optometrist or an ophthalmologist whom you trust. Despite all of the information you’ve found here, none of this is any substitute for actual medical advice, or the care of a health professional who has your best interest and expert-level medical knowledge about your personal anatomy in mind. Also, many other side effects, although rare, are also possible, and only a qualified medical professional will have access to the full suite of information about what you may face. A medical professional will also be able to tell you whether your particular set of circumstances makes you a good candidate for LASIK (or other laser eye surgery options) or not.
Laser vision correction has been a procedure that’s been approved for use in the United States since the mid-1990s, and more than 40 million LASIK procedures have been performed worldwide since its inception, with over half of those procedures occurring within the United States. 700,000 new procedures are performed annually, with an overall patient satisfaction rate of a whopping ~96%, with the largest sources of dissatisfaction being scheduling, cost, and lack of insurance coverage for the procedure, rather than the outcome of the procedure itself. Now that you understand the science behind LASIK and how it works, you can have an informed talk with your doctor and see if it’s right for you!



{kind=link}
{kind=link}
{kind=link}
{kind=link}